
TL;DR: PCOS vs. PCOD
- PCOD (Polycystic Ovarian Disease) is a condition where the ovaries produce immature eggs, often manageable through lifestyle and diet.
- PCOS (Polycystic Ovary Syndrome) is a more serious metabolic and endocrine disorder involving systemic hormonal imbalances and insulin resistance.
- Key Symptoms: Irregular periods, stubborn acne, unexplained weight gain, and hirsutism (excess facial/body hair).
- Diagnosis: Doctors use the Rotterdam Criteria, requiring at least two of three markers: irregular ovulation, high androgen levels, or polycystic ovaries on an ultrasound.
- Prevalence: Affecting approximately 1 in 5 women in India, these conditions are highly linked to insulin resistance (found in 50–70% of cases) and genetic factors.
I hear this almost every week. A woman sits across from me and says, “Doctor, I do not know what is happening to my body anymore.”
Irregular periods, stubborn acne, and weight that will not go away, no matter how carefully she eats. And hair showing up in places it never was before.
She has been told she is stressed, that she should lose weight, or that it will sort itself out. It has not sorted itself out. And she is not imagining it.
If any of that sounds familiar, you may have been living with PCOS or PCOD without ever having a name for it.
This blog is my attempt to give you that name. And more than that, to help you understand what it means for your body, your mind, and your life.
The Scale of This Problem in India
Before we go further, I want you to see the numbers. Because one of the cruelest parts of this condition is how alone it makes women feel.
I have spent more than a decade watching women arrive in my consulting room after years of being dismissed by doctors, by family, by their own voice inside their heads telling them not to make a fuss.
This is for every woman who was told her pain was not real. It is.
What is PCOS and PCOD? Let Me Draw You a Clear Picture
I always draw a distinction when a patient asks me this. People use these two terms interchangeably. They are not the same thing.
PCOD
Polycystic Ovarian Disease
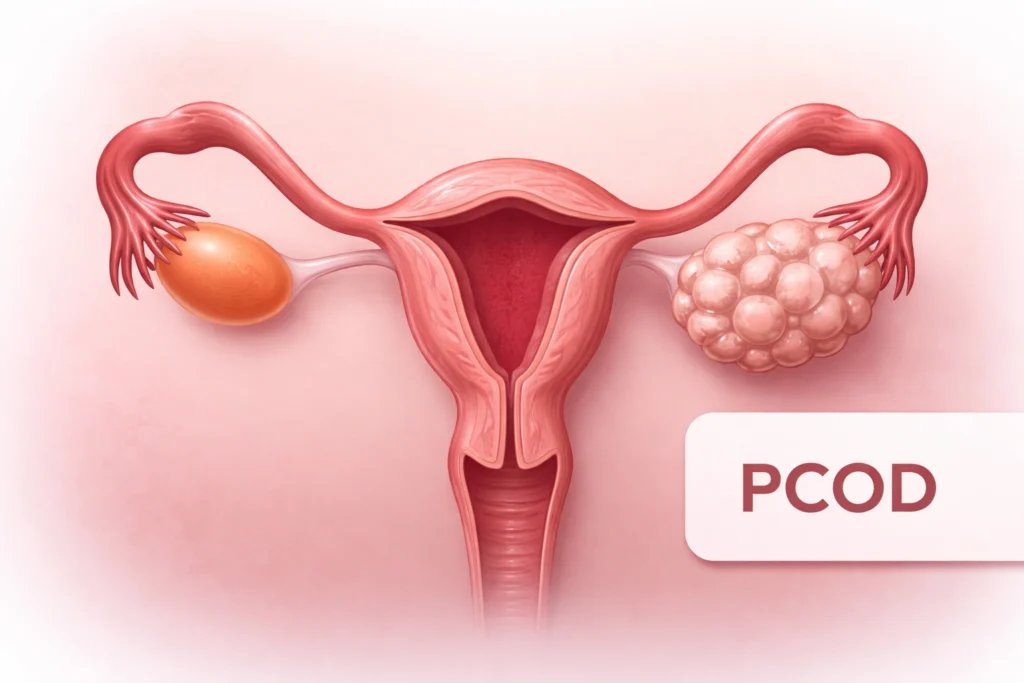
- PCOD is mainly an ovary problem
- Ovaries release immature eggs
- Those eggs do not develop properly
- The Multiple immature eggs in the ovary is mentioned as cysts
- Periods become irregular
- Hormones are mildly affected
PCOS
Polycystic Ovary Syndrome
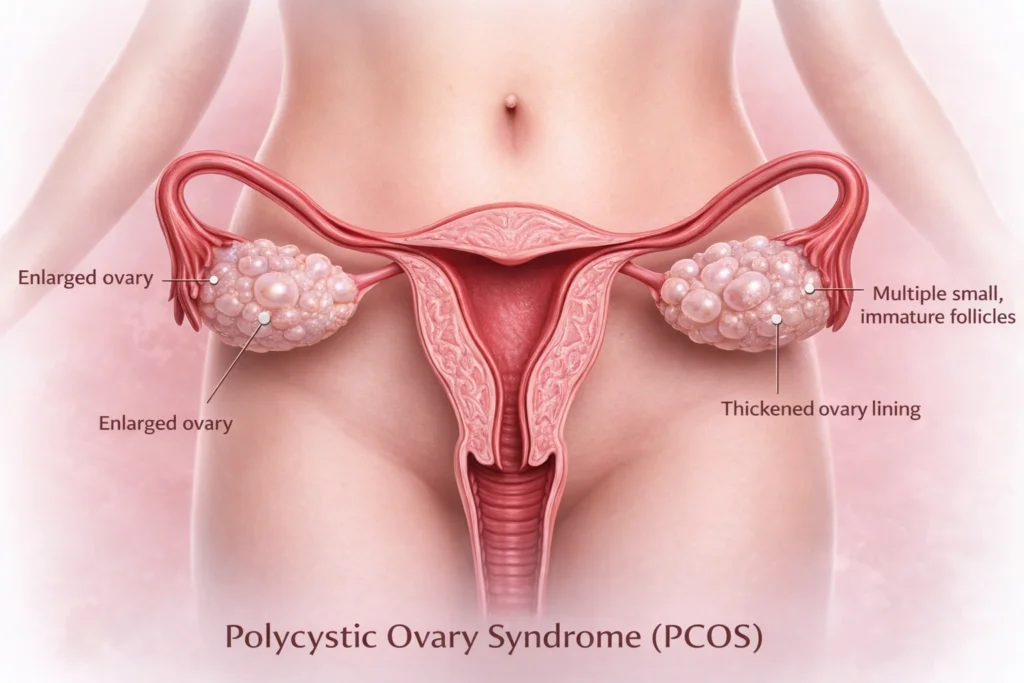
- PCOS is a full-body hormonal condition
- Too many male hormones (androgens) are produced
- Ovulation gets disrupted
- Insulin resistance is very common
- Metabolism is affected
- Multiple body systems are involved
This is for every woman who was told her pain was not real. It is.
Can PCOD develop into PCOS?
While PCOD and PCOS are technically separate diagnoses, they exist on a similar spectrum. If the underlying hormonal and lifestyle issues of PCOD are neglected, they can worsen until the condition effectively meets the criteria for a PCOS diagnosis
Which one is more serious?
Patients ask me this all the time. My answer:
- PCOS carries more long-term risk if unmanaged. Insulin resistance, Type 2 diabetes, and cardiovascular complications are all associated with unmanaged PCOS
- PCOD is generally milder, but it does not get better by itself
- Both conditions require proper investigation, not guesswork
The standard I use in my practice is called the Rotterdam Criteria. It requires that a patient meet at least 2 of 3 specific signs before I confirm a PCOS diagnosis. I will explain those in the diagnosis section.
How Your Body Might Be Telling You
The first thing I want you to understand about symptoms: two women can have the exact same diagnosis and almost no overlapping experiences. This is the nature of PCOS and PCOD. It does not follow a script.
What I am going to share with you is not a checklist to self-diagnose. It is a mirror. Read it and notice what looks familiar.
1. The Periods That Come and Go on Their Own Schedule
The first question I ask any patient when I suspect PCOS or PCOD is: tell me about your periods. It is usually the earliest sign. And the one most women have been quietly worried about for years.

Many women brush this off. They blame a stressful month, a bad diet, travel, and late nights. But when it keeps happening, month after month, your body is not being dramatic. It is sending a signal.
Watch for:
- Irregular periods — cycles shorter than 21 days or longer than 35 days
- Missed periods for weeks or months at a stretch
- Very heavy bleeding when your period does arrive
- Spotting between periods
- Cycles that are completely unpredictable
These are among the most common symptoms of PCOD and early signs of PCOD that women report.
2. The Symptoms You Can See
These are the visible symptoms, the ones that change how a woman moves through the world.
| Symptom | What many of my patients experience |
|---|---|
| Acne or oily skin | Breaking out at 24 or 32 feels different from teenage acne. It sits deep, it is stubborn, and it does not respond to what worked before. |
| Facial or body hair (hirsutism) | Hair on the chin, upper lip, chest, or abdomen. Many women spend years removing it quietly, alone, not knowing it has a clinical name and a clinical cause. |
| Thinning hair on the scalp | Hair loss that starts at the crown. It is distressing and often dismissed as stress or poor nutrition. |
| Weight gain, especially abdominal | Weight that concentrates around the middle even when you are eating carefully. You are then told to simply eat less. That advice misses the point entirely. |
I need to say this directly about weight:
Some women with PCOS gain weight easily and cannot stop. Others struggle to gain any weight at all and are told they cannot possibly have PCOS because they are thin. Both groups are in my waiting room. Both have the diagnosis. PCOS does not have a body type.
3. The Symptoms Nobody Talks About
The symptoms I have to specifically ask about, because patients rarely mention them first, are the invisible ones.
- Fatigue that does not respond to sleep or rest
- Brain fog, which is difficulty concentrating, forgetting things, and feeling mentally slow
- Sugar cravings that feel compulsive, especially in the afternoon
- Mood swings that feel disproportionate to what is happening around you
- Anxiety that has no clear cause and seems to have gotten worse over time
- Low energy that other people around you do not seem to experience in the same way
Remember: You do not need to have every symptom on this list. Many women have two or three. The signs and symptoms of polycystic ovarian disease look different in every woman. That is exactly what makes it so easy to miss and so important to investigate properly.
Why Does PCOS or PCOD Happen?
PCOS has roots in genetics, in the way your body processes insulin, and in hormonal signalling that began long before any lifestyle choice you made.
The first thing I tell a woman after a PCOS diagnosis is this: you did not cause this. It is not because of what you ate, how much you exercised, or how stressed you were.
Understanding why it happens matters.
| Cause | What is happening in the body |
|---|---|
| Hormonal imbalance | Hormonal imbalance and PCOS: elevated androgens disrupt ovulation and trigger skin, hair, and cycle changes |
| Insulin resistance | Cells do not respond to insulin properly. This amplifies androgen production and affects weight and energy. Up to 70% of PCOS patients have insulin resistance. |
| Genetics | A 2024 global survey of Indian women with PCOS found 18% had a family history of PCOS. Sisters were the most commonly affected relative at 66%, followed by mothers at 32%. |
| Lifestyle factors | Chronic stress, poor sleep, and high-sugar diets can worsen existing hormonal imbalance and PCOS. Sedentary behaviour is increasingly linked to rising PCOS prevalence in urban India. |
Because PCOS symptoms vary so much, women often feel they cannot even talk to friends who have the same diagnosis. Your version looks different from hers. Your struggles are not identical. And so even in a shared diagnosis, there can be a deep loneliness.
There is also a particular silence that surrounds this condition in lower-income households and conservative families, where a woman does not go to the doctor because she does not want to explain why. A missed period becomes a source of shame.
In my 15+ years of practice, I have learned that the hardest part of PCOS/PCOD is not the hormones. It is what the hormones do to how a woman feels about herself.
Your experience is valid even if it looks nothing like someone else’s. And you deserve proper care, not just management of your silence.
Struggling with irregular periods or PCOS symptoms?
Located in Tricity, Punjab, Dr Tejinder Kaur offers personalised consultations for women at every stage of their hormonal health journey. You do not need to have all the answers before you come in.
Consult with Dr Tejinder KaurMyths About PCOS and PCOD That Need to Be Addressed
| The myth | The truth | Why it matters clinically |
|---|---|---|
| Only overweight women get PCOS/PCOD | Lean PCOS/PCOD is real and very common. A Mumbai community study found PCOS prevalence of 22.5% regardless of body type. | Thin women are being missed every day because of this assumption. Body size is a possible symptom, not a prerequisite for diagnosis |
| You cannot get pregnant with PCOS/PCOD | Many women with PCOS/PCOD conceive naturally or with minimal support. Fertility is affected, not eliminated. | This fear is carried in silence by thousands of Indian women. It deserves a proper conversation, not a dismissal |
| It is only about your ovaries | PCOS involves insulin resistance, adrenal function, and metabolic health. It is a whole-body condition. | Treating only the ovaries misses the point. The whole system needs attention |
| Regular periods mean you are fine | PCOS/PCOD can exist with regular cycles. Hormonal imbalance does not always stop ovulation. | This assumption delays more diagnoses than any other. Regular bleeding does not rule out PCOS/PCOD |
| It only matters when you want a baby | PCOS/PCOD raises long-term risk of Type 2 diabetes, cardiovascular disease, and endometrial issues | A woman of 25 who is not planning pregnancy still deserves proper management. PCOS is a lifelong condition, not a fertility problem |
| PCOS and PCOD are the same thing | PCOD is mainly an ovarian condition. PCOS is a full-body hormonal syndrome. | Getting the correct diagnosis changes the treatment approach. They are not interchangeable |
How is PCOS or PCOD Diagnosed?
The Rotterdam Criteria
At least 2 of these 3 must be present for a confirmed diagnosis:
- Irregular or absent ovulation, which is seen in your cycle history
- Elevated androgen levels, which is confirmed by symptoms or a blood test
- Polycystic ovaries, which is seen on an ultrasound scan
The number most articles avoid telling you: The current threshold for polycystic ovaries on ultrasound is 20 or more follicles per ovary, or an ovarian volume greater than 10mL. One ultrasound finding alone does not confirm PCOS. It is one part of a three-part picture. Do not interpret your scan results without a doctor.
Tests Performed and Why
| Test | What it checks | Why it matters |
|---|---|---|
| Pelvic ultrasound | Ovarian size, follicle count, cyst presence | Directly confirms or rules out polycystic ovaries. One of the three Rotterdam markers for PCOS diagnosis |
| LH and FSH ratio | Luteinising hormone vs follicle stimulating hormone balance | An elevated LH:FSH ratio is one of the most consistent findings in blood tests for PCOS |
| Free testosterone | Androgenic hormone levels in blood | Tells me whether hyperandrogenism is present. This is Rotterdam criterion 2 |
| Fasting insulin and glucose | How efficiently cells respond to insulin | Up to 70% of PCOS patients have insulin resistance. This is where treatment often begins |
| Thyroid panel (TSH) | Thyroid hormone levels | Thyroid disorders can mimic PCOS symptoms almost exactly. I rule it out before I rule PCOS in |
| Prolactin | Pituitary hormone levels | Elevated prolactin can cause identical symptoms. Including this ensures I am not missing a different diagnosis |
When should you see a doctor?
- You have had irregular periods for 3 or more consecutive cycles
- You have noticed significant changes in hair growth, skin, or weight without a clear cause
- You have been trying to conceive for more than 6 months without success
- You have a mother or sister with PCOS or PCOD, and recognise these symptoms in yourself
How to Manage PCOS or PCOD after Diagnosis

Conclusion
PCOS and PCOD are not death sentences. They are not signs that your body has failed you. They are conditions with names, with pathways, and with real management options.
Before you leave this page:
- If you recognise your symptoms here: write them down. Dates, patterns, changes. That list is your first appointment.
- If you have a mother or sister with PCOS or PCOD: tell your doctor, even if you feel fine
- If you have been dismissed before: you are allowed to ask again. You are allowed to see a different doctor.
- If you are struggling emotionally: that is part of the condition, not a separate weakness. Say that out loud in your next appointment
If this feels like your story, it might be time to have a conversation with someone who takes it seriously.
Book an Appointment at Dr Tejinder Kaur’s Clinic in Tricity, Punjab, Today.
Frequently Asked Questions
Q1: What is the difference between PCOS and PCOD?
PCOD is primarily an ovarian condition where immature eggs do not develop properly and collect as cysts. PCOS is a broader hormonal and metabolic disorder affecting the entire body, including insulin regulation and androgen levels. The PCOD and PCOS difference matters for treatment: PCOS typically requires more comprehensive management because it affects multiple systems, not just the ovaries. Both conditions are real and both require proper investigation.
Q2: How do I know if I have PCOS?
You will not know for certain without a clinical assessment. What I tell patients is this: if you have two or more of the following, see a doctor.
- Irregular cycles that have persisted for 3 or more months.
- Acne that does not respond to standard treatment.
- Unexplained weight changes or hair changes.
- Family history of PCOS.
This is how to know if you have PCOS or PCOD as a starting point. A clinical assessment with blood tests and an ultrasound is what confirms it.
Q3: Is PCOD common in India?
Extremely common and significantly underdiagnosed. Globally, the prevalence is estimated at 1 in 5 to 1 in 10 women of reproductive age. In India, rising numbers are linked to dietary shifts, stress, and lifestyle changes alongside existing genetic predisposition.
Q4: Can I get pregnant with PCOS?
Yes, and I say that confidently, having supported many PCOS patients through successful pregnancies. PCOS makes ovulation less predictable, which can make conception more challenging. But less predictable is not impossible. Many women with PCOS conceive naturally. Those who need support have genuinely good options available. The earlier you speak to a doctor, the more options remain open to you.
Q5: Is PCOD curable permanently?
Neither PCOD nor PCOS is curable in the conventional medical sense. But it can be managed so effectively that it stops running your life. With the right lifestyle approach and medical support sustained over time, the majority of women achieve significant symptom reduction and a full quality of life.
Q6: Which test is done for PCOD and PCOS?
No single test confirms either condition. A PCOS diagnosis test panel typically includes LH/FSH ratio, free testosterone, fasting insulin, thyroid function (TSH), and prolactin, alongside a pelvic ultrasound. All results are considered together with your symptom history. Anyone who offers a diagnosis from one test alone is not working to the clinical standard.
Q7: Can I have PCOS with regular periods?
Yes. PCOS can coexist with regular or near-regular cycles because hormonal imbalance does not always prevent ovulation entirely. This is among the most important myths to correct. Regular bleeding does not rule out PCOS. If you have other symptoms and a family history, please do not let a regular calendar be the reason you do not get investigated.